Let's get started
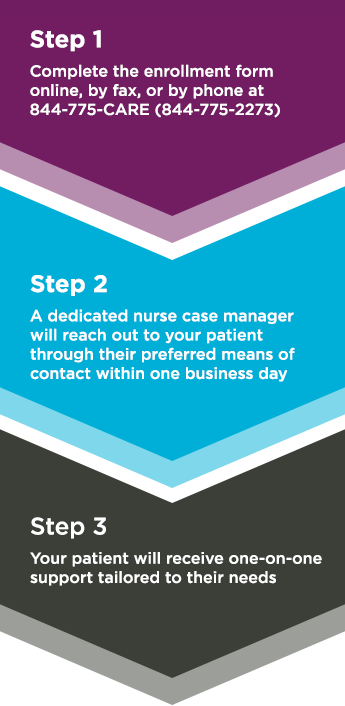
We are ready to help you. A dedicated nurse case manager will work directly with US patients for one-on-one support. They can answer questions about treatment planning.

(For US residents only)
(For US residents only)

We focus on making enrollment quick and easy.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088 (1-800-332-1088).
Call a dedicated
nurse case manager
We’re ready to help walk you through the enrollment process.
Available Monday-Friday, 9 AM-7 PM (EST)
To receive benefits under the KIMMTRAK CONNECT Co-pay Support Program (“Program”), the patient must enroll into the Program and attest the patient meets the eligibility criteria and agrees to and will comply with the terms and conditions described below:
KIMMTRAK is a prescription medicine used to treat HLA-A*02:01-positive adults with uveal melanoma that cannot be removed by surgery or has spread.
What is the most important information I should know about KIMMTRAK?
KIMMTRAK can cause serious side effects that can be severe or life threatening and usually happen within the first three infusions, including:
Tell your healthcare provider right away if you get any of these symptoms. Your healthcare provider will check for these problems during treatment with KIMMTRAK. Your healthcare provider may temporarily stop or completely stop your treatment with KIMMTRAK if you have severe side effects.
See "KIMMTRAK can cause other serious side effects" for more information.
Before receiving KIMMTRAK, tell your healthcare provider about all of your medical conditions, including if you:
Tell your healthcare provider about all medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements.
These are not all the side effects possible with KIMMTRAK.
Call your healthcare provider for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088 (1-800-332-1088).
Please read the accompanying Patient Information Leaflet before you receive KIMMTRAK and discuss any questions you have with your healthcare provider.
Please see KIMMTRAK Patient Information.
Immunocore, KIMMTRAK, and KIMMTRAK CONNECT are registered trademarks of Immunocore Ltd. All other trademarks, company and product names, and logos are the property of their respective owners.
©2025 Immunocore Ltd. All rights reserved.
CM-US-TEBE-2100039 v14.0 December 2025
Immunocore, KIMMTRAK, and KIMMTRAK CONNECT are registered trademarks of Immunocore Ltd. All other trademarks, company and product names, and logos are the property of their respective owners.
©2025 Immunocore Ltd. All rights reserved.
CM-US-TEBE-2100039 v14.0 December 2025